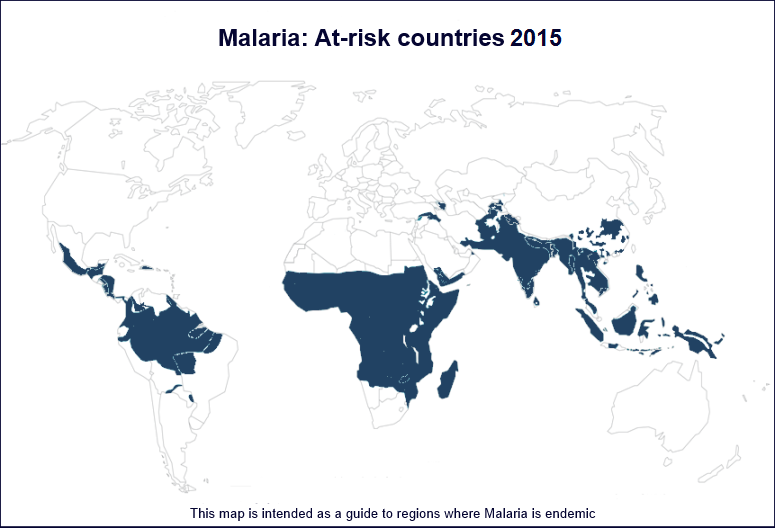
Malaria: Malaria Tablets
You can argue that Malaria is a disease in decline, with year-on-year reductions in both infections & mortality since
the year 2000, yet Malaria continues to be a disease of Biblical proportions: there were 1200 malaria Deaths per day in 2015 - mainly African children.
Malaria has been known to man for millennia, the word originates from Medieval Italian: mala aria — "bad air", which was thought to be the cause of the disease.
Malaria 'peaked' in the 1800's when European trade and colonisation in the tropics were marked by enormous losses of life from the disease.
The first major breakthrough
in the treatment of Malaria was the drug Quinine, which was derived from the bark of the Cinchona tree in southern Peru.
Symptoms of malaria include fever and flu-like illness, including headache, tiredness, nausea, muscle aches, vomiting, and diarrhoea.
For most people, symptoms begin 10 days to 4 weeks after being bitten, although symptoms can emerge
much later, up to 1-2 years in extreme cases.
As a backpacker, you are unlikely to die from Malaria, but I
know of plenty of people that have caught it - invariably it's those
travellers who are lackadaisical about the preventative measures who end
up being infected, e.g. people who stop taking their medication for some spurious reason, or
who are too vain to cover-up in the evenings or when
mosquitoes are in the air.
There is no vaccination (injection) for Malaria, you'll need to
take a course of prophylactic (preventative) tablets before, during
and after your stay in an at-risk country. There are a number of
different drugs available and your doctor or travel clinic will recommend
one for you based on where you're headed, your length of stay and your
medical history (see below).
When I first visited Africa (Mid-1990's), Malaria medication consisted of 2 sets of tablets:
Chloroquine & Paludrine,
one taken daily, one weekly, with both tasting like dirt. Taking a strict
daily/weekly regimen of pills is difficult to do when you're on the road, it's
easy to miss a day when you're not feeling 100% or when your medication is buried in the bottom of your pack. You are unlikely to be offered
Chloroquine
today as the malaria parasite has developed resistance to the drug in some
parts of the world.
All anti-malarial drugs have some common attributes -
firstly they're expensive, secondly no prophylactic (preventative) drug is
100% effective in preventing malaria, and thirdly the side-effects;
all the main drugs have side-effects of one sort or another,
usually
quite mild, e.g. a stomach upset. Most travellers don't have any issues, but if you are
concerned, you should start your course of tablets well ahead of your
departure date (i.e. while you're at home) and deal with any issues
before you leave, your doctor will be OK with this and you'll have time to
switch to an alternative medication if needed.
Three of the more common anti-malarial drugs in use today are described
below:
Larium (aka Mefloquine) is the oldest of the three drugs I'm going to talk about
here, Larium's main advantage is that the dosage is one tablet per week,
a big plus-point because it's much easier to cope with a weekly regimen
when you're on the road. The downside of Larium is the side-effects
experienced by some travellers are more severe (your travel clinic will
tell you more). The side effects are real, but only a very small minority
of users are affected. IMO Larium gets a bad rap in general and is blamed
for anything & everything on the road... I have used Larium on 3 trips with no issues,
in fact the only side-effect I encountered was acute nausea from listening to
whinging backpackers blaming the drug for everything from their altitude
sickness to relationship breakdown to global warming. Another disadvantage
of Larium is the long 'overlap' required, you need to start taking your
course of tablets 2 weeks before you enter an infected country/area and
for 4 weeks after you leave, so you'll probably be using the drug for
quite a while.
Doxycycline is one of the cheaper anti-malarials, the dosage is a
single tablet taken daily, starting just 2 days before you enter an
infected country/area and for 4 weeks after you leave, the most
significant side-effect is increased sensitivity to bright sunlight.
Doxycycline is also used to treat acne.
Malarone is the new anti-malarial 'kid' on the block and it's the
most expensive, it's a combination of 2 drugs (Atovaquone/Proguanil) and has fewer side-effects
than other anti-malarials. Malarone is taken daily starting two days
before you enter an infected country/area and for just seven days
after you leave, this short 'overlap' makes the drug suitable for those
people travelling in and out of infected areas, i.e. where you would stop
taking the medication at some point, then start again when re-entering an
infected area. The downside of Malarone is firstly the cost and secondly because it is a new'ish
drug, it's unproven for long-term use (long-term=months).







